
Future-Proofing Healthcare Starts with Emotional Intelligence
At a glance:
- Emotional intelligence (EI) doesn’t just develop with time, targeted efforts accelerate meaningful growth
- EI is a critical skill to build in healthcare, supporting performance, patient care, and staff well-being under pressure
- With the right measurement, EI development becomes visible, trackable, and actionable—not just theoretical
Healthcare professionals work in environments that are as meaningful as they are demanding, requiring not only clinical expertise, but also compassion, collaboration, and resilience under pressure. In this context, emotional intelligence (EI)—the set of emotional and social skills that shape how we understand ourselves, relate to others, and navigate challenges—has gained increasing attention as a potential support for both performance and well-being among healthcare teams.
While this would suggest that healthcare students and practitioners should learn and develop EI, it leads us to an important question: Do EI development efforts actually work? Is it worthwhile to spend time developing EI, and if so, what do effective development efforts look like?
Why EI is Important in Healthcare
EI plays an important role in healthcare performance. Higher EI has been linked to stronger in-role performance (such as work accuracy), extra-role contributions (like supporting colleagues), and adaptive performance (including managing stress and navigating complex situations), as well as lower levels of counterproductive behavior (e.g., disengagement or lack of motivation).¹
Beyond performance, EI is also associated with a range of positive professional behaviors, including effective leadership, creativity, conflict management2, and resilience.3 It has also been linked to “deep acting” forms of emotional labor, where individuals align their internal emotional responses with job expectations—for example, generating genuine empathy in patient interactions.²
Despite these well-documented benefits, EI is not always recognized as a meaningful solution to misconduct or skill gaps. For instance, analyses of disciplinary cases across 21 state dental boards found that many infractions were linked to deficits in EI rather than cognitive or technical ability.⁴ This disconnect is notable, particularly given evidence that EI can support practitioners’ work by improving care quality and patient satisfaction5, while also enhancing their well-being.
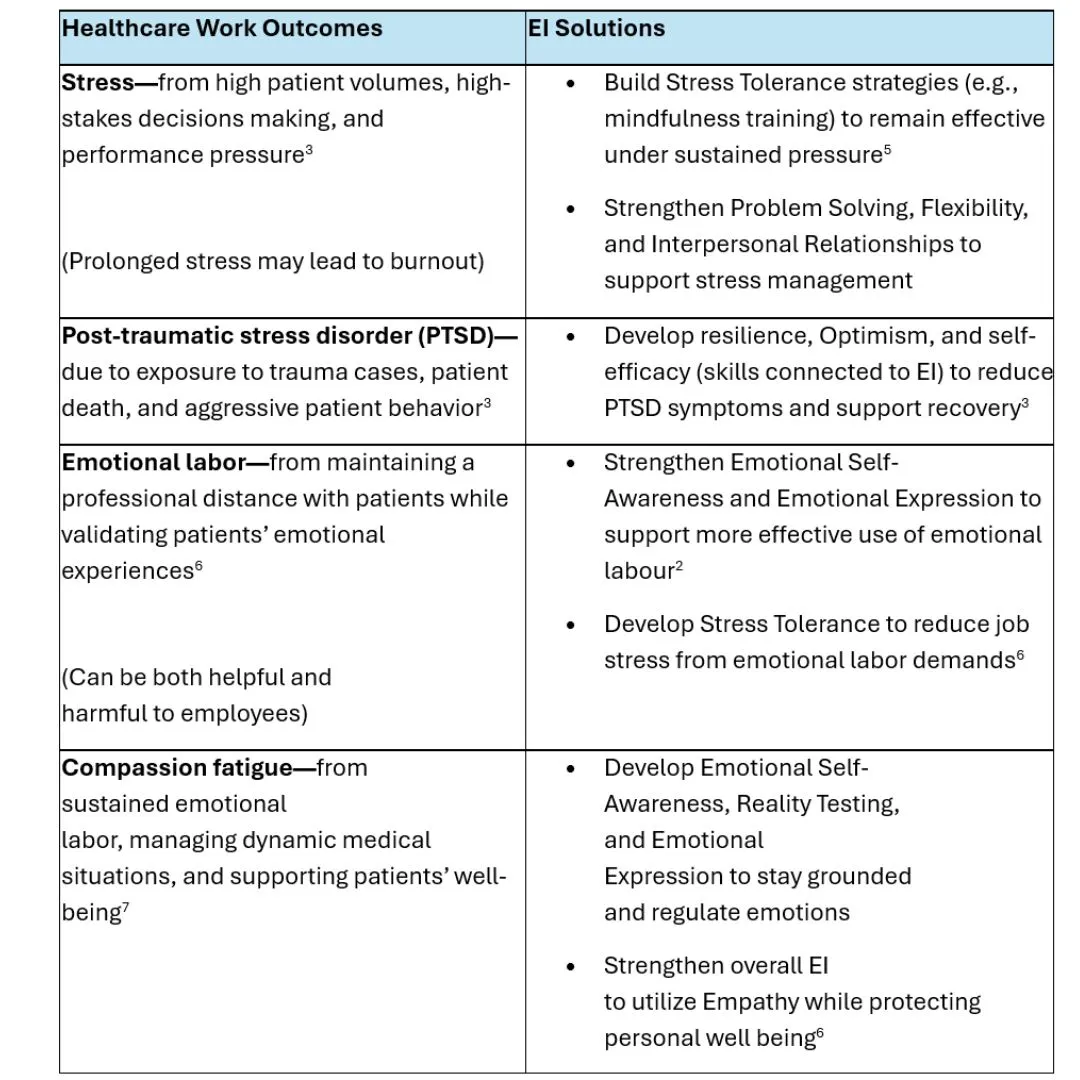
There are multiple ways EI can help mitigate the impact of the demands on healthcare workers:
Why Measuring Change Matters for EI
Skills aren’t fixed—they can be developed over time through experience, reflection, and practice.
One way to better understand and build these skills is through tools like MHS’ Emotional Quotient Inventory 2.0 (EQ-i 2.0®). The assessment helps connect core EI skills to real-world situations, making it easier to identify strengths, uncover opportunities for growth, and take targeted action. It provides a structured view of EI with an overall EI score, as well as five key areas, each broken down into more specific skill sets (subscales) to guide development priorities.
When it comes to development, it’s important to distinguish between improvement that happens naturally over time and improvement that results from intentional effort. While research shows that EI tends to increase with age and life stage⁸, this doesn’t necessarily tell us whether specific training or interventions lead to meaningful change within individuals over time.
That’s where evidence becomes critical. By understanding which approaches actually lead to measurable improvements in EI, healthcare organizations can focus their time, resources, and training efforts where they will have the greatest impact. In a field where time is limited and demands are high, this kind of insight helps ensure that development efforts are not only well-intentioned but effective.
How EI Development Works in Healthcare
A growing body of research has examined the effectiveness of EI development in healthcare using the EQ‑i 2.0. Across studies published since 2016, healthcare professionals and students completed the EQ‑i 2.0 before and after targeted interventions. Although the programs and timelines varied, the findings were consistent: EI skills improved meaningfully over time.
Learning Through Experience
One way EI develops is through immersive, real-world experiences.
For example, studies in dental⁹ and therapy programs¹⁰,¹¹ found that clinical placements (where students regularly navigate stress, make complex decisions, and interact with patients) led to significant increases in Total EI scores as well as skills such as Self-Regard, Self-Actualization, Independence, Problem Solving, Reality Testing⁹,¹⁰, Impulse Control⁹, and Stress Tolerance.¹⁰
Similarly, research on hyper-realistic surgical simulation training for military medical students showed that high-pressure, unpredictable scenarios can accelerate EI development. These simulations required adaptability, collaboration, and rapid decision-making, and resulted in significant gains in Total EI and subscales scores³,⁵, with particularly strong improvements in Self-Perception and Stress Management.³,⁵ Happiness scores (and the connected subscales) also significantly increased⁵, suggesting students felt more confident and prepared in their roles.
Taken together, these findings show that experience-based learning—especially in realistic or high-pressure environments—can strengthen EI skills while also building professional confidence and readiness.
Learning Through Targeted EI Programs
EI can also be developed through structured programs designed to directly build specific skills.
For instance, one study introduced an “Emotional Intelligence–Resilience” elective for medical students, covering topics such as optimism, reframing, reflection, and meaning, and combining these with applied assignments, such as self-reflection essays¹²,¹³. Other approaches focused on core EI competencies such as self-awareness, self-management, social awareness, and social skills through group discussions¹⁴, while others involving medical students¹⁵ and hospital staff16 incorporated individual or group assessment, mentoring, and roleplay-based learning. Across these approaches, results were consistent: participants showed significant increases in Total EI12–16, subscale, and Happiness scores, showing the strongest improvements in Self-Perception, Self-Expression, and Stress Management skills.12–14
Beyond score improvements, participants described gaining a better understanding of EI’s value in healthcare, greater confidence in developing EI, and stronger skills for managing stress and burnout.12 They also noted responding with more patience and consideration, handling conflict more effectively, and a stronger sense of team pride and shared responsibility for team well-being.16 These insights reinforce the practical value of EI development in healthcare settings.
Across studies, several clear patterns emerge:
- Consistent increases in Total EI
- Strong gains in Stress Management and related skills
- Improvements in self-confidence (e.g., Self-Regard, Independence)
- Realistic expectations of workplace demands (e.g., Reality Testing)
- Increased ability to manage pressure (e.g., Stress Tolerance, Flexibility)
- Gains in overall well-being and Happiness scores
- Engaging, relevant, and applicable qualities of training content
Why This Matters for the EQ‑i 2.0
Across these studies, the EQ-i 2.0 played a critical role in capturing and quantifying change over time.
By measuring EI before and after development—and, in some cases, comparing participants to similar individuals who did not receive intervention¹⁰,¹—the EQ‑i 2.0 demonstrated that meaningful improvement is driven by intentional development efforts, not just time alone.
This provides strong evidence that the EQ‑i 2.0 can be used to:
- Track progress over time
- Evaluate the impact of development programs
- Identify where to focus future training efforts
For healthcare organizations, this makes EI development more than a theoretical goal; it becomes something that can be measured, managed, and continuously improved.
Learn more about the relationship between emotional intelligence and healthcare
References
1 van Lill, X., Stols, A., Hayes, C., Rajab, P., & Wiggett, J. (2025, March 5). Case study: Emotional Quotient Inventory® 2.0 (EQ-i® 2.0) and individual work performance. JVR Africa Group & MHS.
2 Saha, S., Das, R., Lim, W. M., Kumar, S., Malik, A., & Chillakuri, B. (2023). Emotional intelligence and leadership: Insights for leading by feeling in the future of work. International Journal of Manpower, 44(4), 671–701. https://doi.org/10.1108/IJM-12-2021-0690
3 White, A., Zapata, I., Lenz, A., Ryznar, R., Nevins, N., Hoang, T. N., Franciose, R., Safaoui, M., Clegg, D., & LaPorta, A. J. (2020). Medical students immersed in a hyper-realistic surgical training environment leads to improved measures of emotional resiliency by both hardiness and emotional intelligence evaluation. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.569035
4 Munk, L. K. (2016). Implications of state dental board disciplinary actions for teaching dental students about emotional intelligence. Journal of Dental Education, 80(1), 14-22. https://doi.org/10.1002/j.0022-0337.2016.80.1.tb06053.x
5 West, E., Singer-Chang, G., Ryznar, R., Ross, D., Czekajlo, M., Hoang, T., Alson, R., Berbel, G., Moloff, A., Safaoui, M., Nevins, N., & LaPorta, A. J. (2020). The effect of hyper-realistic trauma training on emotional intelligence in second year military medical students. Journal of Surgical Education, 77(6), 1422–1428. https://doi.org/10.1016/j.jsurg.2020.04.020
6 Karimi, L., Leggat, S., Donohue, L., Farrell, G., & Couper, G. (2013). Emotional rescue: The role of emotional intelligence and emotional labour on well-being and job-stress among community nurses. Journal of Advanced Nursing, 70. https://doi.org/10.1111/jan.12185
7 d’Ettorre, G., Pellicani, V., & Ceccarelli, G. (2020). Post-traumatic stress disorder symptoms in healthcare workers: A ten-year systematic review. Acta Biomed for Health Professions, 91(Suppl 12), e2020009. https://doi.org/10.23750/abm.v91i12-S.9459
8 Shaw, J. (2025, May 1). What We Know: Managing Generation Z in the Workplace. Multi-Health Systems (MHS). https://mhs.com/blog/what-we-know-managing-generation-z-in-the-workplace/
9 Farah-Franco, S. M., Taylor, L. C., Rowan, S. Z., & Andrews, E. A. (2023). A 10-year longitudinal study of dental students’ emotional intelligence and the impact of COVID-19. Journal of Dental Education, 87(12), 1692–1704. https://doi.org/10.1002/jdd.13364
10 Gribble, N., Ladyshewsky, R. K., & Parsons, R. (2017). Fluctuations in the emotional intelligence of therapy students during clinical placements: Implication for educators, supervisors, and students. Journal of Interprofessional Care, 31(1), 8–17. (120327695). https://doi.org/10.1080/13561820.2016.1244175
11 Gribble, N., Ladyshewsky, R. K., & Parsons, R. (2019). The impact of clinical placements on the emotional intelligence of occupational therapy, physiotherapy, speech pathology, and business students: A longitudinal study. BMC Medical Education, 19(1), 90. https://doi.org/10.1186/s12909-019-1520-3
12 Versel, J. L., Plezia, A., Jennings, L., Sontag-Milobsky, I., Adams, W., & Shahid, R. (2023). Emotional intelligence and resilience “PROGRAM” improves wellbeing and stress management skills in preclinical medical students. Advances in Medical Education and Practice, 14, 1309–1316. https://doi.org/10.2147/AMEP.S437053
13 Jennings, L. N., Feffer, M., & Shahid, R. (2024). Sustained impact of an emotional intelligence and resilience curriculum for medical students. Advances in Medical Education and Practice, 15, 1069–1077. https://doi.org/10.2147/AMEP.S488410
14 Shahid, R., Stirling, J., & Adams, W. (2018). Promoting wellness and stress management in residents through emotional intelligence training. Advances in Medical Education and Practice, 9, 681–686. https://doi.org/10.2147/AMEP.S175299
15 Dugan, J. W., Weatherly, R. A., Girod, D. A., Barber, C. E., & Tsue, T. T. (2014). A longitudinal study of emotional intelligence training for otolaryngology residents and faculty. JAMA Otolaryngology–Head & Neck Surgery, 140(8), 720–726. https://doi.org/10.1001/jamaoto.2014.1169
16 Tadmor, T., Dolev, N., Attias, D., Lelong, A., & Rofe, A. (2016). Emotional intelligence: A unique group training in a hematology-oncology unit. Education for Health, 29(3), 179–179. https://doi.org/10.4103/1357-6283.204221

















