
Leveraging hardiness to combat pandemic-related anxiety and depression
The importance of mental health is a topic that is increasingly being discussed in the media and in daily conversations amongst friends, family, and at work. As a result of the COVID-19 pandemic, mental health issues have gained a lot of attention globally, especially anxiety and depression.
A recent review of 47 studies found that 77% of these studies noted a significant relationship between the pandemic and anxiety symptoms, whereas another 56% reported a significant relationship with depression symptoms (Machado et al., 2020). Increases in anxiety and depression may be explained through fears of the virus itself, as well as through the impacts of pandemic restrictions, which have resulted in social isolation, confinement, loss of regular activities, and financial issues.
How does hardiness serve as a protective factor against stress?
While the pandemic challenged many people in many ways, some were able to navigate it without experiencing or exacerbating mental health issues. One factor that may have contributed to this is a person’s psychological hardiness.
Hardiness is a personality factor or mindset that contributes to resilience under stress (Eschleman et al., 2010; Stein & Bartone, 2020). The core components of hardiness are control (“I can influence life outcomes”), commitment (“I have a purpose in life”), and challenge (“Life changes are something to be overcome”). Past research has shown hardiness to be a protective factor against occupational stress in a variety of roles, including executives (Maddi & Kobasa, 1984), nurses (Abdollahi et al., 2014), police (Allison et al., 2019), and military personnel (Bartone, 1999; Britt et al., 2001). Thus, hardiness may also act as a protective buffer between the stressors of the COVID-19 pandemic and their effect on mental health, specifically for anxiety and depression.
To examine this relationship, MHS and Dr. Paul Bartone conducted a study to determine whether hardiness moderated the impact of COVID-19 stress on anxiety and depression, such that individuals with lower hardiness would be expected to have greater anxiety or depression given higher levels of COVID-19 stress (Bartone et al., 2022). This post is based on the outstanding work of Dr. Bartone and colleagues, and the study is described below.
394 Canadian adults completed measures of hardiness, anxiety, depression, COVID-19 related stress, and demographic questions in an online survey. Individuals were screened for attentiveness and data quality, which left 363 people in the sample. The sample was 48.8 years old on average (standard deviation of 15.3 years), and was approximately 50% female, approximately 70% not a visible minority, and approximately 63% employed.
Hardiness was assessed using one of our own assessments, the Hardiness Resiliency Gauge (HRG), which has excellent evidence of reliability and validity (Bartone et al., 2022). Anxiety and depression were assessed using the General Anxiety Disorder-7 (GAD-7; Spitzer et al., 2006) and Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001), respectively; note, these measures are ratings scales, and endorsement of symptoms do not necessarily entail a clinical diagnosis. The COVID-19 stress measure examined the pandemic’s impact (better, worse, or the same, as compared to pre-pandemic) on eight life domains, including: employment stability, work performance, family relationships, friend relationships, physical health, mental health, and education. Correlations between scores on each of the measures were computed, and relationships were further explored using a regression analysis.
Our results showed that anxiety and depression were both positively related to COVID-19 stress (correlations ranged from .29 to .31, representing modest effects), meaning that people who experienced higher levels of COVID-19 stress also reported feeling more anxiety and depression. Conversely, hardiness was moderately negatively associated with anxiety, depression, and COVID-19 stress (correlations ranged from -.27 to -.38), suggesting that people with higher levels of hardiness experienced lower levels of anxiety, depression, and COVID-19 stress.
These relationships were further explored, with hardiness being modelled as a moderator of the COVID-19 stress-to-depression/anxiety relationship. It was revealed that hardiness moderated the relationship between COVID-19 stress and anxiety and depression. Therefore, hardiness can act as a psychological buffer, changing the amount of influence that COVID-19 stress has on people’s levels of anxiety and depression. Individuals with lower hardiness scores experienced greater increases in anxiety or depression symptoms in response to COVID-19 stress, as compared to people with higher hardiness. Individuals with higher hardiness scores showed reduced associations between COVID-19 stress and anxiety and depression.
Figure 1. The moderating effect of hardiness on the relationship between COVID-19 stress and Anxiety (a) and Depression (b).
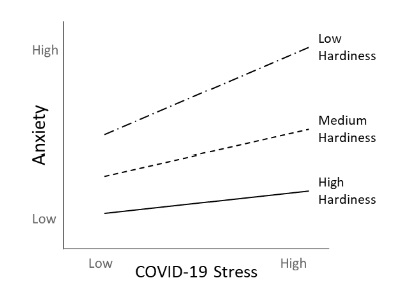
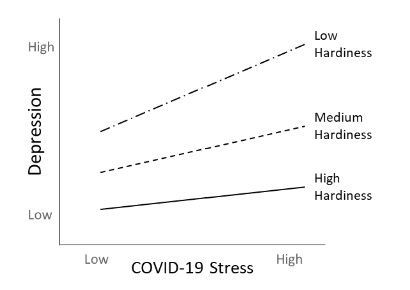
Note. These figures show the relationship between COVID-19 stress and anxiety (a) and depression (b). The lines depict how that relationship changes for people with different amounts of hardiness. The key takeaway is that people with high hardiness show a much flatter line; that is, hardiness serves as a buffer because it reduces the relationship between COVID-19 stress and anxiety and depression.
What is it about hardiness that allows it to act as a buffer for the effects of stress?
The benefits of hardiness start with how hardy people view challenging or disruptive situations in life. They tend to see these situations as being just another part of life and as something to be overcome. When dealing with these situations, active, problem-solving strategies are employed, rather than avoidance coping techniques, such as denial or substance abuse (Bartone & Homish, 2020; Thomassen et al., 2018). Thus, hardy people put a positive spin on things, tackle their problems head on, and do their best to adapt to new realities.
The good news is that hardiness can be developed with proper training. Coaching targeting any of the three components of hardiness (control, commitment, and challenge) can influence overall hardiness. (Bartone et al., 2016; Judkins et al., 2006).
Further, workplaces can foster hardiness among employees by promoting and role-modelling positive coping strategies during stressful times, allowing workers to have greater control over their tasks and schedules, and providing recognition for a job well done (Bartone, 2017). Increasing hardiness in employees is associated with reduced symptoms of anxiety and depression and can also potentially mitigate the stress of unprecedented events, like the COVID-19 pandemic, and its effects on mental health.
Learn more about how MHS’ Hardiness Resiliency Gauge (HRG) may be used to develop your team in ways that will protect them against burnout and stress.
References
Abdollahi, A., Abu Talib, M., Yaacob, S. N., & Ismail, Z. (2014). Hardiness as a mediator between
perceived stress and happiness in nurses. Journal of Psychiatric and Mental Health Nursing,
p21(9), 789–796.
Allison, P., Mnatsakanova, A., McCanlies, E., Fekedulegn, D., Hartley, T. A., Andrew, M. E., & Violanti, J.
M. (2019). Police stress and depressive symptoms: Role of coping and hardiness. Policing, 43(2),
247–261.
Bartone, P. T. (1999). Hardiness protects against war-related stress in Army reserve forces. Consulting
Psychology Journal, 51(2), 72–82.
Bartone, P.T. (2017). Leader influences on resilience and adaptability in organizations. In U. Kumar, The
Routledge International Handbook of Psychosocial Resilience (pp. 355–368). Routledge.
Bartone, P. T., Eid, J., & Hystad, S. W. (2016). Training hardiness for stress resilience. In N. Maheshwari
&, V. V. Kumar, Military Psychology: Concepts, Trends and Interventions (pp. 231–248). Sage.
Bartone, P. T., & Homish G. G. (2020). Influence of hardiness, avoidance coping, and combat exposure
on depression in returning war veterans: a moderated-mediation study. Journal of Affective
Disorders, 265, 511–518.
Bartone, P. T., McDonald, K., Hansma, B. J., & Solomon, J. (2022). Hardiness moderates the effects of
COVID-19 stress on anxiety and depression. Journal of Affective Disorders, 317, 236-244.
Bartone, P. T., McDonald, K., Hansma, B. J., Stermac-Stein, J., Escobar, E. M. R., Stein, S. J., & Ryznar, R.
(2022). Development and validation of an improved hardiness measure: the Hardiness
Resilience Gauge. European Journal of Psychological Assessment.
Britt, T. W., Adler, A. B., & Bartone, P. T. (2001). Deriving benefits from stressful events: the role of
engagement in meaningful work and hardiness. Journal of Occupational Health Psychology, 6,
53–63.
Eschleman, K. J., Bowling, N. A., & Alarcon, G. M. (2010). A meta-analytic examination of hardiness.
International Journal of Stress Management, 17(4), 277–307.
Judkins, S. K., Reid, B., & Furlow, L. (2006). Hardiness training among nurse managers: building a healthy
workplace. Journal of Continuing Education in Nursing, 37, 202–207.
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ‐9: Validity of a brief depression severity
measure. Journal of General Internal Medicine, 16(9), 606–613.
Machado, D. B., Alves, F. J. O., Teixeira, C. S. S., Rocha, A. S., Castro-de-Araujo, L. F. S., et al. (2020).
Effects of COVID-19 on anxiety, depression and other mental health issues: a worldwide scope
review. Research Square, 1–53.
Maddi, S. R., & Kobasa, S. C. (1984). The hardy executive. Jones-Irwin.
Spitzer, R.L., Kroenke, K., Williams, J.B., & Löwe, B. (2006). A brief measure for assessing generalized
anxiety disorder: the GAD-7. Archive of Internal Medicine, 166(10), 1092–1097.
Stein, S. J., & Bartone, P. T. (2020). Hardiness: Making stress work for you to achieve your life goals.
Wiley.
Thomassen, Å. G., Hystad, S. W., Johnsen, B. H., Johnsen, G. E., & Bartone, P. T. (2018). The effect of
hardiness on PTSD symptoms: A prospective mediational approach. Military Psychology, 30(2),
142–151.









