Untangling ADHD, Anxiety, Trauma, and Mood in Assessment
At a glance:
- ADHD, anxiety, trauma, and mood disorders can present with a striking symptom overlap, but the underlying drivers (and treatments) are not the same.
- Surface symptoms rarely tell the full story; patterns across context, time, and informants are what differentiate.
- When the differential is unclear, better data—not more symptom checklists—is what leads to accurate diagnosis.
Attention-deficit/hyperactivity disorder (ADHD) is rarely a straightforward diagnosis. Many of its hallmark features, like executive dysfunction, impulsivity, and emotional dysregulation are not unique to ADHD but also cut across anxiety disorders, trauma- and stressor-related conditions, and mood disorders, often strongly enough to complicate even careful clinical evaluation.1 As a result, the diagnostic question is rarely a clean “is this ADHD?” It is more often: is this ADHD alongside another condition, or is another condition producing an ADHD-like clinical picture?
That distinction matters enormously for treatment. Anxiety, depression, trauma-related disorders, and ADHD may share overlapping symptoms while requiring very different intervention approaches. When symptoms are misattributed, individuals may spend years receiving treatment that addresses a visible presentation without targeting the underlying mechanism that is driving impairment.
Comorbidity further complicates the picture. More than half of both adults and children with ADHD have at least one comorbid psychiatric disorder, with rates in adults reported as high as 80% in some studies.1-5 Anxiety, trauma- and stressor-related conditions, and mood disorders are among the most common overlapping presentations. Pure diagnostic profiles are the exception rather than the rule, making differential diagnosis both common and clinically challenging.
When symptom overlap is this substantial, accurate differential diagnosis cannot rely on symptom counts alone. Standardized, norm-referenced assessment becomes clinically important because it helps clinicians move beyond surface-level similarities to examine symptom patterning, context, developmental course, functional impairment, and cross-informant consistency.
The Overlap Problem
At the core of the challenge is that many commonly observed difficulties, such as executive dysfunction and emotional dysregulation, are not unique to ADHD. These are transdiagnostic processes, meaning they appear across a range of conditions, each with different underlying causes and treatment implications.5
This complexity is compounded by comorbidity. Co-occurring conditions often interact with one another in ways that make presentations harder to disentangle. For example, anxiety can further impair executive functioning, while ongoing difficulties with attention and regulation can contribute to increased anxiety, creating a reinforcing cycle that amplifies both.6 In some cases, stress, depression, or anxiety may also emerge as downstream consequences of undiagnosed or untreated ADHD, rather than independent primary conditions. In practice, clinicians are often evaluating intertwined presentations rather than clean diagnostic categories.
Diagnostic bias adds another layer of complexity. Women and girls with ADHD disproportionately present with internalizing symptoms that are often interpreted primarily as anxiety or depression, contributing to systematic under-identification of ADHD in females.7
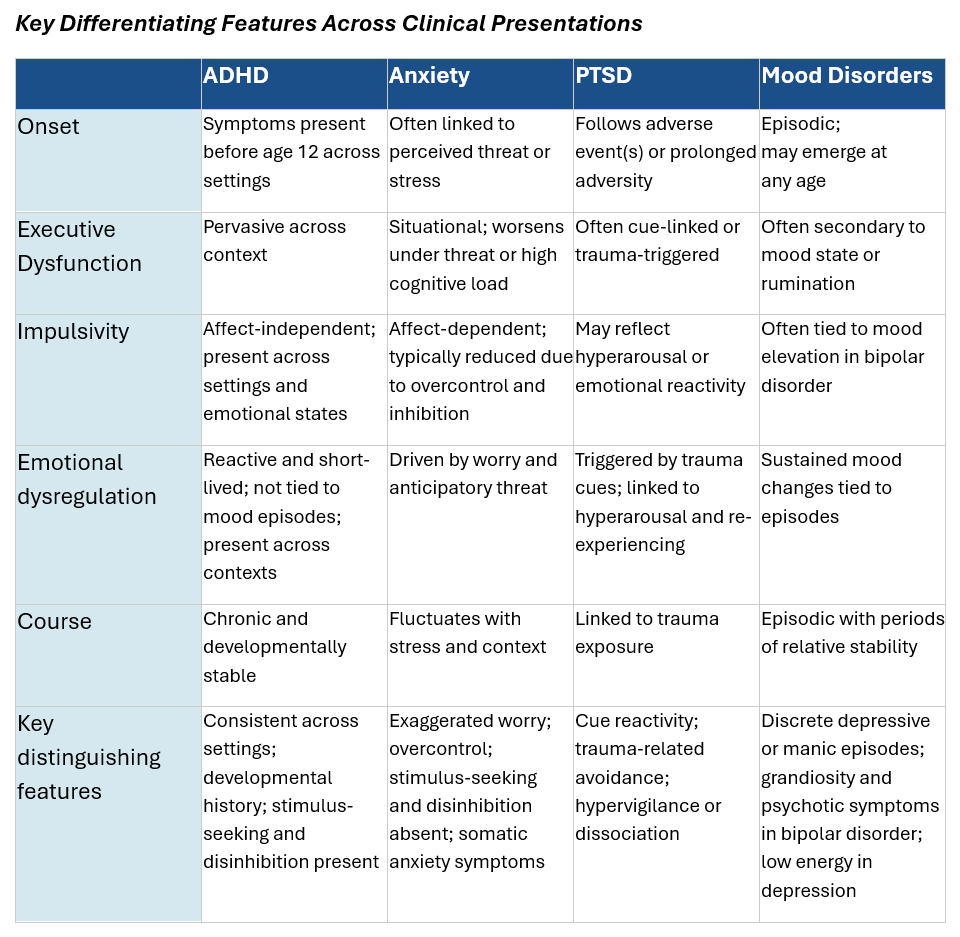
Key differentiating features of ADHD and common comorbidities1,5,8,9; ADHD = Attention-deficit/hyperactivity disorder; PTSD = Post-traumatic stress disorder
ADHD and Anxiety Disorders
ADHD and anxiety disorders share meaningful overlap in both presentation and underlying cognitive systems, that govern attention regulation and behavior control.2
Research suggests there may be multiple pathways to this overlap. In some individuals, ADHD-related executive dysfunction generates secondary anxiety as individuals struggle to meet demands they cannot reliably regulate. In others, severe anxiety produces enough cognitive load that it mimics executive dysfunction despite intact underlying neurodevelopmental functioning.8
For clinicians, the key question becomes: what is driving the observed difficulty? Several signals can help differentiate these presentations.
Context matters. In ADHD, executive dysfunction tends to be present across settings, regardless of emotional state. In anxiety, difficulties are more situational, emerging in high-pressure or perceived threat contexts.
Impulse control also differs. Anxiety is typically associated with overcontrol and heightened inhibition, whereas ADHD is characterized by disinhibition and stimulus-seeking behaviour.8,5
These distinctions matter clinically because both presentations can produce similar surface-level symptoms, including inattention, restlessness, and emotional distress. Anxiety and ADHD also have distinct treatment approaches, and misidentifying which is primary has direct consequences for what gets prescribed and in what order.5
ADHD and Trauma
ADHD and post-traumatic stress disorder (PTSD) share substantial overlap in executive dysfunction, impulsivity, emotional dysregulation, and hyperarousal.9 Individuals with ADHD are also at greater risk of developing PTSD following traumatic events, and co-occurrence is associated with greater illness severity and psychosocial dysfunction.10
Onset and developmental history are critical signals. ADHD symptoms must be present before age 12 and occur across multiple settings, independent of specific stressors. In contrast, trauma-related symptoms emerge following adverse experiences, even when those experiences are not immediately disclosed.
Context can also help differentiate. ADHD-related attentional difficulties tend to be relatively consistent across situations, whereas trauma-related difficulties are often cue-linked and intensify in the presence of reminders or perceived threat. An added challenge is that trauma histories are frequently undisclosed, particularly in school-based or early clinical evaluations. As a result, comprehensive developmental history and trauma-informed screening are essential components of any ADHD assessment.
These distinctions matter because similar outward behaviours may reflect very different underlying mechanisms. Without accounting for trauma, clinicians risk misinterpreting stress responses as neurodevelopmental deficits, leading to incomplete formulations and less effective intervention planning.
ADHD and Mood Disorders
Mood disorders, like major depression and bipolar disorder, can also resemble ADHD, particularly in adults. Irritability, emotional dysregulation, and difficulties with executive functioning appear across all three conditions.2, 6
The key differentiator is clinical course: mood disorders involve distinct periods of significant difficulty followed by relative stability, while ADHD is chronic and developmentally consistent.2 In bipolar disorder, cyclical mood elevation, grandiosity, and psychotic symptoms during episodes are not features of ADHD, even during periods of high impulsivity or restlessness.2 Individuals with primary ADHD can experience repeated failures and setbacks and may become demoralized, presenting with what looks like depression. In these cases, treating mood symptoms without addressing underlying ADHD may produce incomplete improvement.5
A Framework for Effective Differential Assessment
When ADHD, anxiety, trauma-related disorders, and mood disorders present with overlapping symptoms, effective differential diagnosis depends on integrating multiple sources of structured information rather than relying on symptom counts alone.
Standardized, norm-referenced assessments, like the Conners 4th Edition™ (Conners 4®) and Conners Adult ADHD Rating Scales™ 2nd Edition (CAARS™ 2) support this process by capturing patterns of symptom expression across domains that align with different diagnostic possibilities. Several features are particularly critical when selecting and interpreting assessment:
- Multi-informant data: Differences across raters (home, school, self-report) help distinguish pervasive vs. context-dependent patterns. ADHD is typically consistent across settings; anxiety and trauma often vary by context.
- Developmental history and chronicity: ADHD requires early-onset and chronic course, while trauma-related symptoms follow adverse experiences and mood disorders are episodic, making the establishment of timing critical for diagnosis.
- Functional impairment across domains: Understanding where impairment occurs (e.g., school, relationships, daily functioning) helps clarify the underlying condition.
- Scale-level interpretation: Differential diagnosis depends on the pattern of elevations across scales rather than any single scale score. How attention, impulsivity, mood, and anxiety features shape the overall profile is what clarifies the diagnosis.
Research highlights the importance of this profile-based approach. One study found that a combination of CAARS subscales, including Hyperactivity, DSM-Inattention, and the ADHD Index, alongside depression symptom severity correctly classified 88% of participants across ADHD and MDD groups, with hyperactivity emerging as a key differentiator between ADHD and MDD specifically.1
Findings from the Conners 4 norm sample similarly highlight the value of profile-level interpretation. Emotional dysregulation was elevated across youth with ADHD, anxiety, and depression, reflecting a symptom dimension that cuts across these conditions. Differentiation emerged in the broader profile: the ADHD group showed greater elevations on Hyperactivity and Impulsivity, while the anxiety and depression groups showed higher elevations on Anxious Thoughts and Depressed Mood.¹¹ The full profile captures both what these conditions share and what sets them apart.
The Cost of Getting It Wrong
The overlap between ADHD and anxiety, trauma, and mood disorders is well established—and the cost of getting it wrong is high. When underlying drivers are missed, treatment may address symptoms without resolving their source. When comorbid conditions are overlooked, the clinical picture remains incomplete.
In high-demand systems, there is understandable pressure to move quickly from symptoms to diagnosis. But when presentations overlap, accuracy depends on more than pattern recognition. It requires structured, multi-informant data that captures how symptoms unfold across contexts and time, because getting the picture right is what determines whether treatment works.
Explore how to strengthen your differential assessment approach. Get in touch with our team.
Want more insights like this delivered to your inbox? Subscribe to receive the latest articles, research, and resources from MHS.
References
¹ Paucke, M., Stibbe, T., Huang, J., & Strauss, M. (2021). Differentiation of ADHD and depression based on cognitive performance. Journal of Attention Disorders, 25(7), 920–932. https://doi.org/10.1177/1087054719865780
² Katzman, M. A., Bilkey, T. S., Chokka, P. R., Fallu, A., & Klassen, L. J. (2017). Adult ADHD and comorbid disorders: Clinical implications of a dimensional approach. BMC Psychiatry, 17, Article 302. https://doi.org/10.1186/s12888-017-1463-3
³ Ohnishi, T., Kobayashi, H., Yajima, T., Koyama, T., & Noguchi, K. (2019). Psychiatric comorbidities in adult attention-deficit/hyperactivity disorder: Prevalence and patterns in the routine clinical setting. Innovations in Clinical Neuroscience, 16(9–10), 11–16.
⁴ Guo, Y., Li, J., Hu, R., Luo, H., Zhang, Z., Tan, J., & Luo, Q. (2024). Associations between ADHD and risk of six psychiatric disorders: A Mendelian randomization study. BMC Psychiatry, 24, Article 99. https://doi.org/10.1186/s12888-024-05548-y
⁵ Canadian ADHD Resource Alliance (CADDRA). (2011). Canadian ADHD practice guidelines (3rd ed.). CADDRA.
⁶ Fu, X., Wu, W., Wu, Y., Liu, X., Liang, W., Wu, R., & Li, Y. (2025). Adult ADHD and comorbid anxiety and depressive disorders: A review of etiology and treatment. Frontiers in Psychiatry. https://doi.org/10.3389/fpsyt.2025.1597559
⁷ Attoe, D. E., & Climie, E. A. (2023). Miss. Diagnosis: A systematic review of ADHD in adult women. Journal of Attention Disorders, 27(7), 645–657. https://doi.org/10.1177/10870547231161533
⁸ Alarachi, A., Merrifield, C., Rowa, K., & McCabe, R. E. (2024). Are we measuring ADHD or anxiety? Examining the factor structure and discriminant validity of the Adult ADHD Self-Report Scale in an adult anxiety disorder population. Assessment, 31(7), 1508–1524. https://doi.org/10.1177/10731911231225190
⁹ Magdi, H. M., Abousoliman, A. D., Ibrahim, A. M., Elsehrawy, M. G., EL-Gazar, H. E., & Zoromba, M. A. (2025). Attention-deficit/hyperactivity disorder and post-traumatic stress disorder adult comorbidity: A systematic review. Systematic Reviews. https://doi.org/10.1186/s13643-025-02774-7
¹⁰ https://doi.org/10.1177/1087054723116153310. Biederman, J., Petty, C. R., Spencer, T. J., Woodworth, K. Y., Bhide, P., Zhu, J., & Faraone, S. V. (2013). Examining the nature of the comorbidity between pediatric attention deficit/hyperactivity disorder and post-traumatic stress disorder. Acta Psychiatrica Scandinavica, 128(1), 78–87. https://doi.org/10.1111/acps.12011
¹¹ Conners, C. K. (2022). Conners 4th Edition (Conners 4) [Manual]. Multi-Health Systems, Inc.